





Why Do Augmented Breasts Look So “Augmented” or Fake?
In this weeks edition of “Why Does Everyone Look So Weird?” I will examine the obstacles to attaining what so many women want in a breast augmentation: A scarless full youthful look that doesn’t have “plastic surgery” written all over it. The obvious “augmented look” is rampant and well tolerated by the public and celebrities alike and I am sure some readers will be thinking right now “but I like the augmented look better than the natural look.” I am the first person to say that I am not the plastic surgeon for everyone but I will say that even when patients come to my office with that mindset they nearly always leave with a complete reorientation wanting a natural looking augmentation. The problem lies in understanding what a beautiful natural look is. Most think natural means low and flat and augmented means full. When I show patients requesting an augmented look pictures of the widely separated overly round and low “augmented look” and pictures of my results which have gentle slopes without harsh edges and separation I almost always get a “no no no that’s what I want response.”
Call (305) 328-8256 to schedule a consultation with Dr. Rian Maercks to learn more about breast augmentation.

The Augmented Look vs The Natural Look in Breast Augmentation
Augmented look vs Natural look
Before getting deep into this issue, I will flatly say that my thoughts about breast augmentation and breast aesthetics are VERY contraculture to the mainstream conceptions and standards of my field. It is my opinion that many practices in medicine and plastic surgery are very dogmatic. I find the well accepted aesthetics of the augmented breast very disappointing even though this is a very high patient satisfaction procedure. Not everyone will understand, relate to or agree with what I write here. I am unwilling to intentionally deliver unnatural appearing results to the face breast or body. I perform 100% subfascial breast augmentation, I perform 100% transaxillary (through the armpit) in primary breast augmentations that do not require lifting and I use 100% low profile anatomically shaped implants. These three components are aberrations from mainstream plastic surgery..
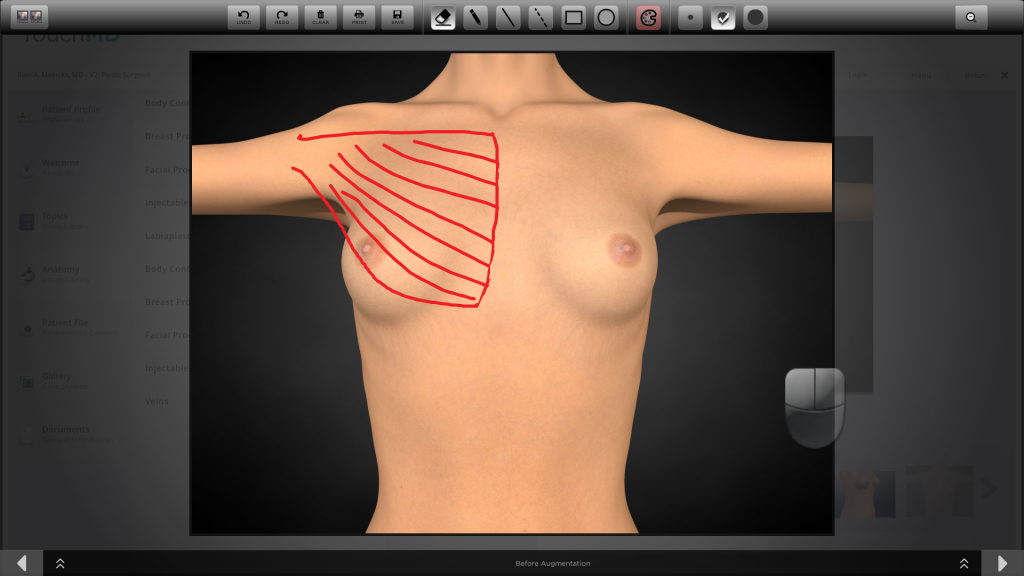
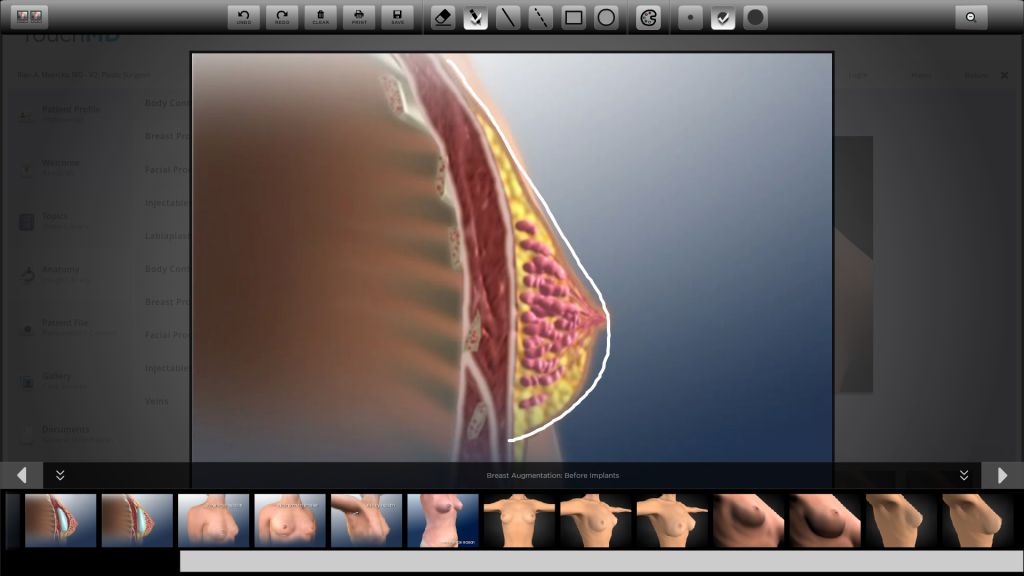
Here we go… I find a great starting point for understanding mainstream breast augmentation is to use one of the tools developed by expert plastic surgeons and industry partners, a software platform called TouchMD. It is a convenient tool with patient education diagrams and videos that one can draw on in consultation. I will use screen shots from this system to illustrate my points. Forgive the preschool looking drawings and writing displayed as this is not a high accuracy fine art system. Below see the first illustration in the breast augmentation section, a picture titled “before breast augmentation”:
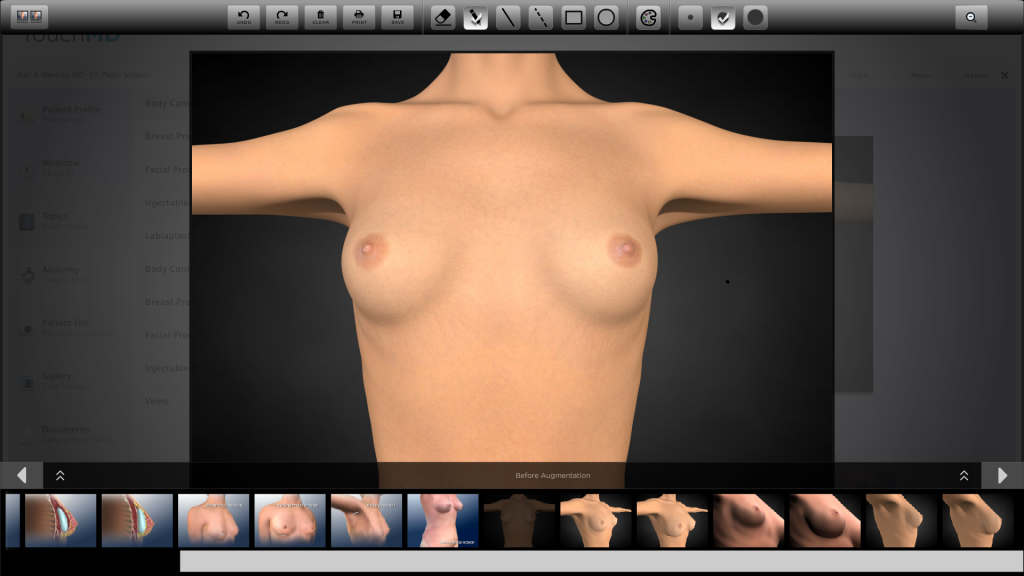
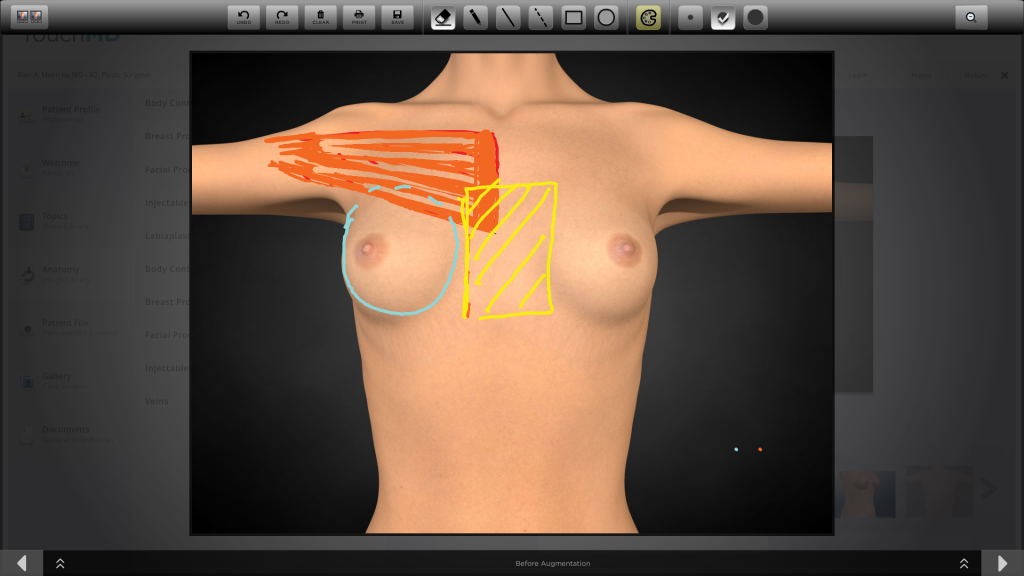
“Before breast augmentation.”
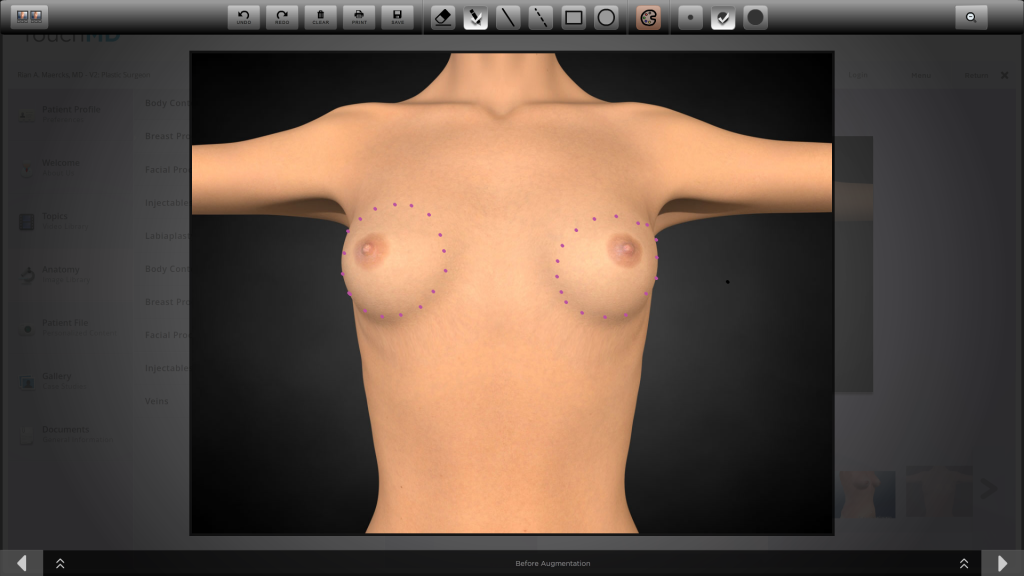
Does the picture above look like a pair of natural breasts to you? It certainly doesn’t look like any natural pair of breasts that I have ever seen. Lets look at why. First of all they are round like balls:
There is also a ridiculously large space between them. They are very far from midline demonstrated by the orange hashed space:
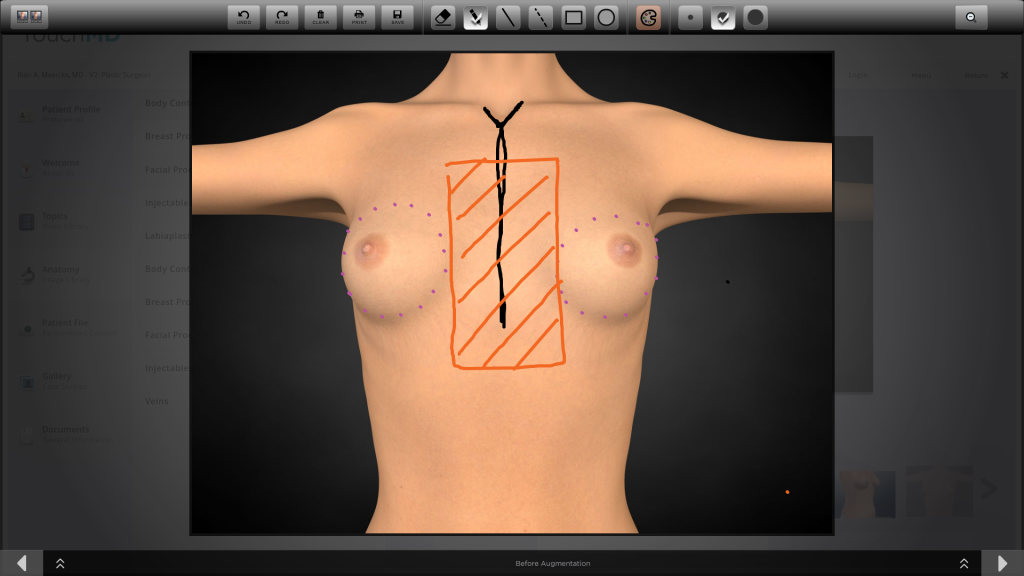
In fact it is not hard to imagine fitting a third breast between them. If you are old enough to remember the movie Total Recall this will look familiar:
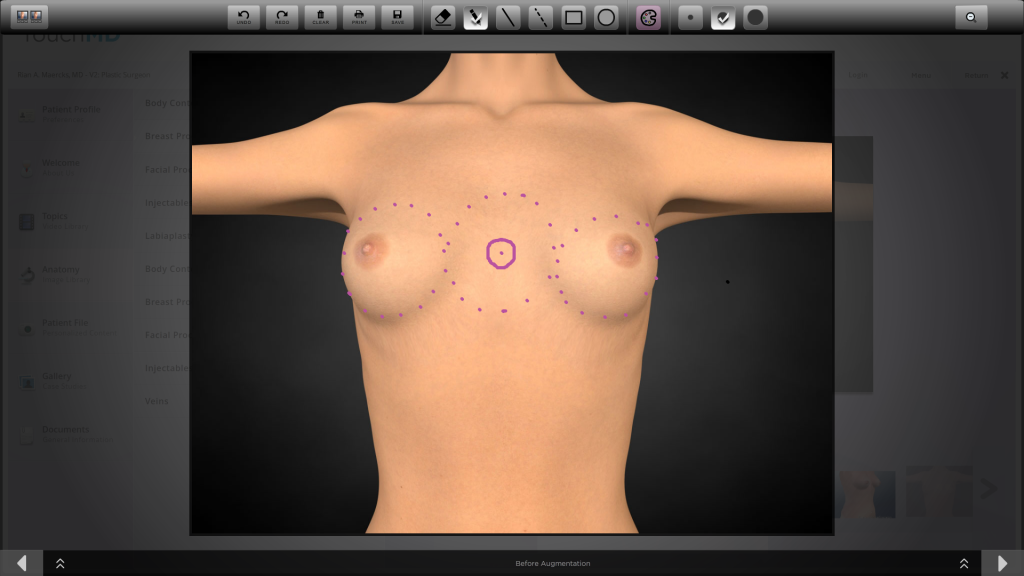
So now we are left with the question: Why would a team of expert plastic surgeons and this company produce a very expensive practice enhancing software suite with such a ridiculous representation of normal untouched breast anatomy?!?!
My simple answer: This is the now accepted norm for “augmented breasts” and the aesthetics of submuscular high profile implants have become the standard aesthetic goal for most plastic surgeons.
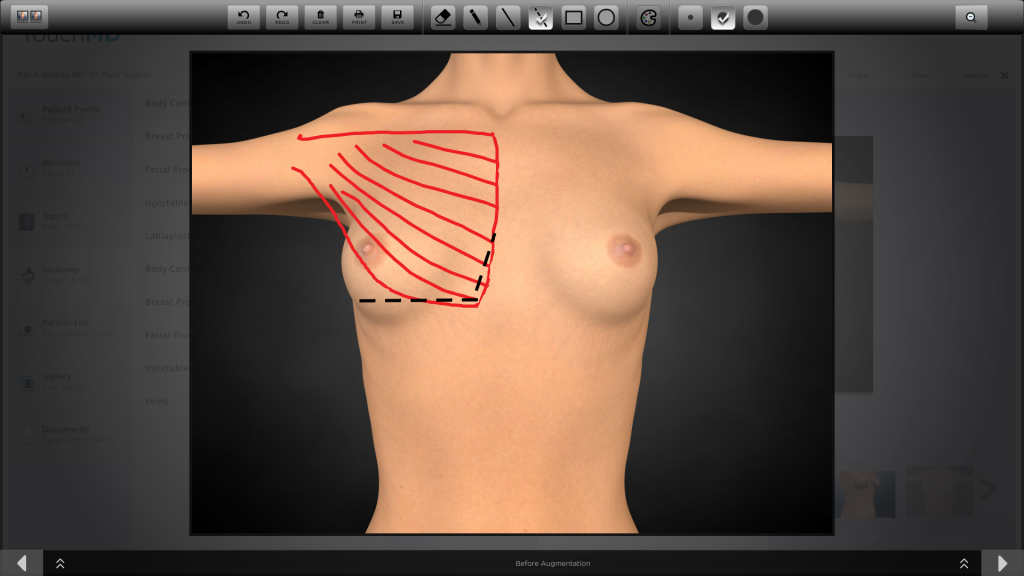
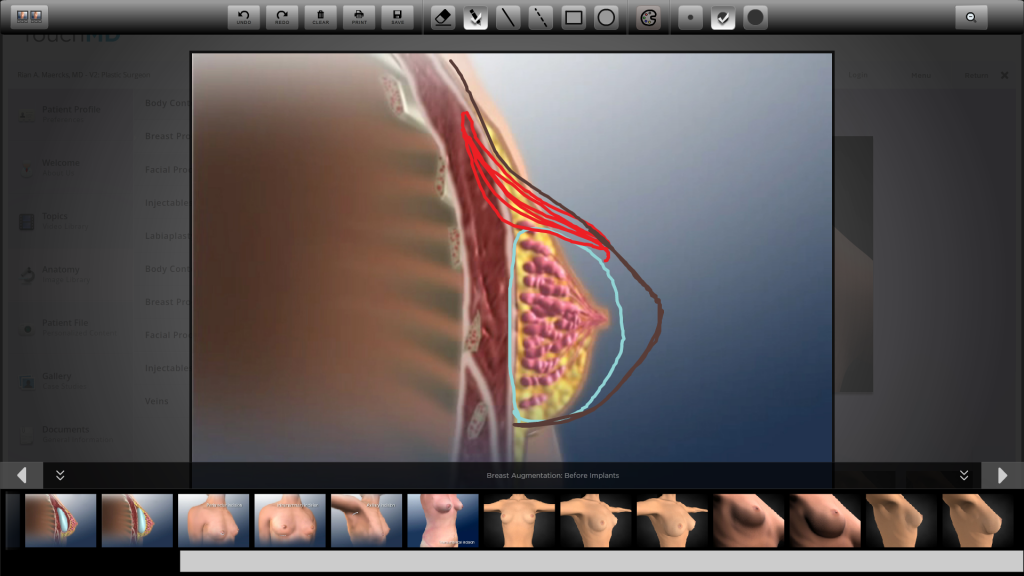
Lets take a look at why and how this has happened. The most commonly used type of breast augmentation procedure in the United States is what the public calls “under the muscle” and what surgeons call “dual-plane.” The pectoralis major muscle natively exists in a position and shape roughly as sketched below:
In a conventional “dual-plane breast augmentation, the inferior attachments and much of the midline attachments of the pectoralis major muscle are destroyed as the black dotted lines depict below:
The muscle then “window-shades” upwards as depicted by the orange shape below:
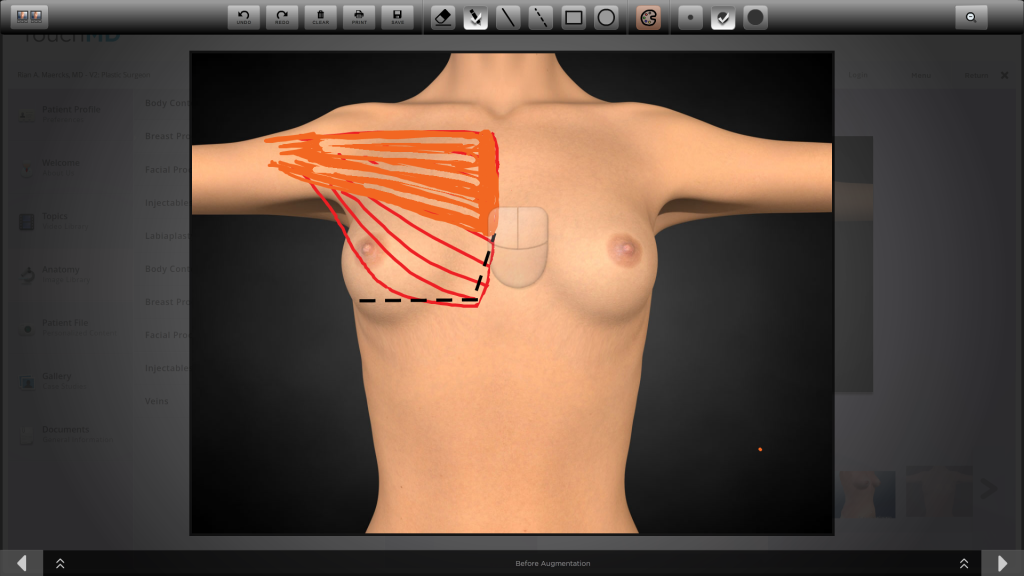
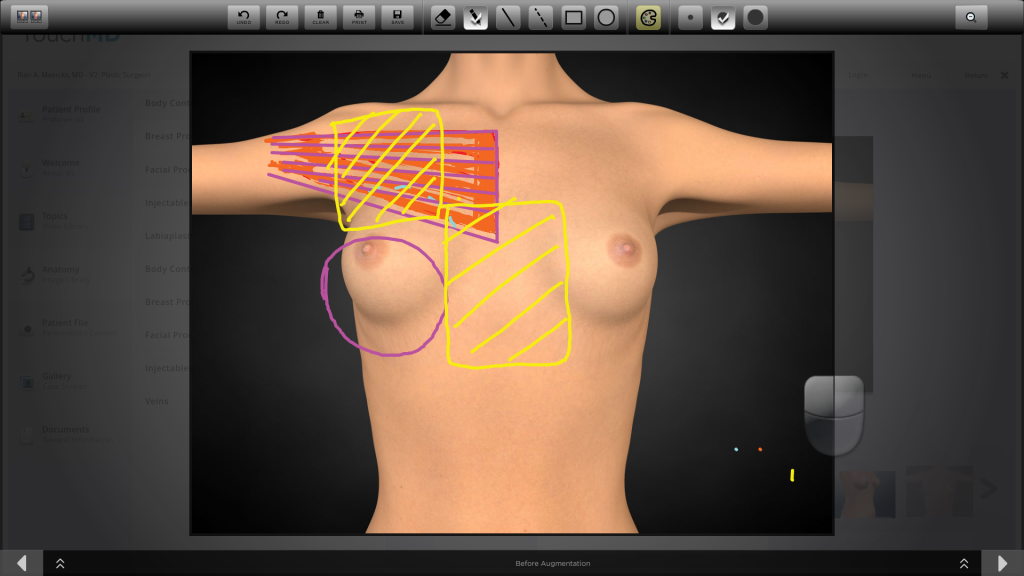
We will cover implant selection and why surgeons select implants that will create a fake look in depth later but for now we will just leave it at the fact that 90%+ of augmentations in this country are performed with moderate to high profile round breast implants. With the dual-plane submuscular approach, the remaining origination attachments of the muscle prevent the implant from approaching midline, and the implant ends up exactly where this illustration depicts a “natural” breast existing as demonstrated below.
This separation leads to the wide flat sternal space so commonly seen in breast augmentation, what we jokingly refer to as “The Miami Valley” as seen in the yellow hatched box below.
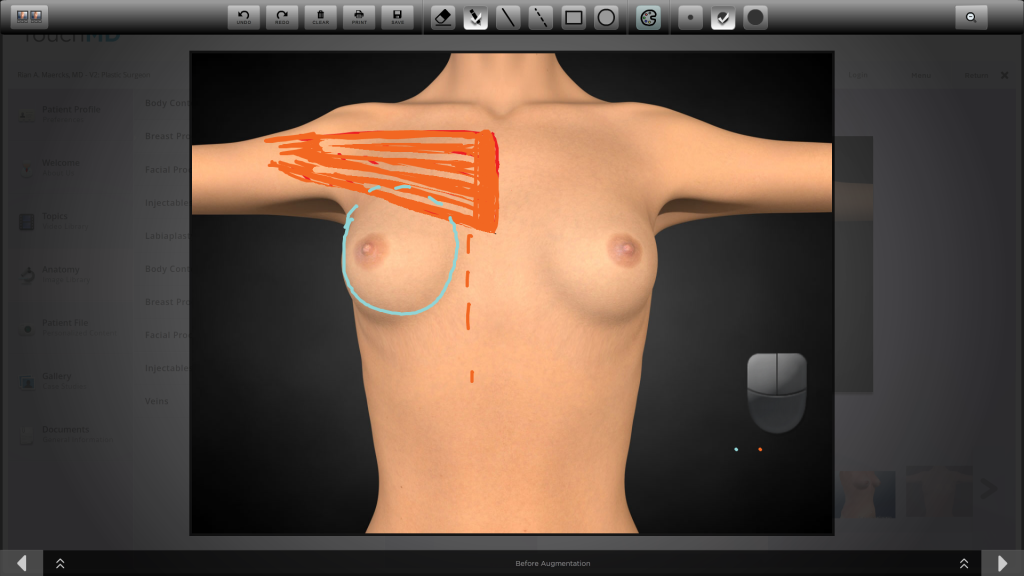
It is however important to realize that the pectoralis major muscle is not a floating pad that is likely to create a blended soft breast, it is a muscle!!! It is an important muscle that participates in most movements of daily life and arm stabilization. As such it ALWAYS has tone unless we are sleeping or dead, thus like a rope pulled taught will quickly return to the shortest distance between its origination and insertion. In the case of the pectoralis major muscle, this means the chest wall. What does this mean for the implant? Further downward and outward displacement as illustrated below:
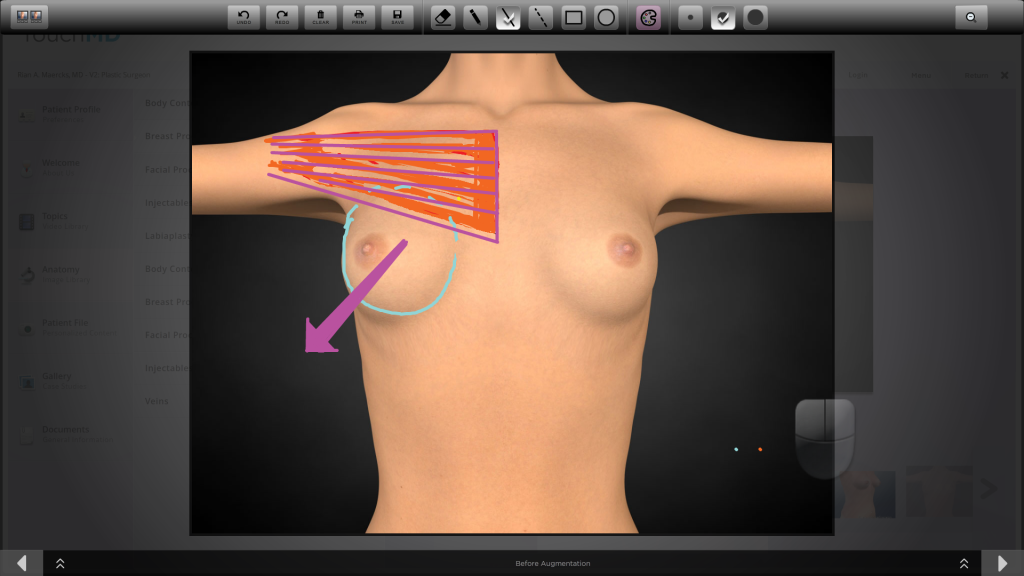
Forces in the sub muscular or dual-plane breast augmentation technique lead to widening and inferolateral implant malposition.
The return of the muscle towards chest wall leads over time to an implant falling towards the armpit and down with a completely flat central and upper chest unless the patient is wearing a supporting and lifting garment. Thus the flat superior pole, shelf like appearance of the top of the implant and the widely separated look has become the halmark “augmented” look until further progression of these forces over time cause a “rock in a sock look.”
The resulting “augmented look” is a narrow projecting breast accentuated by surrounding contrast of flatness
Now lets realize that although these features describe most augmentation results out there, most women are pretty happy with them. Mostly they look good in clothes and the breasts are bigger. Most women accept the rest. I believe this is true because they are unaware of other options.
Lets again look at this in real life. The patient below did not come to me for breast concerns. She was a model and a facial aesthetics patient of mine. One day she was in the office and said “its been almost two years since my breast augmentation can you take a look so I dont have to go back to my other surgeon.” I of course obliged her. When I examined her I told her that she had a good result for whats out there but in my practice I found the result to be unacceptable. We discussed what I do and the aesthetics I try to obtain with a technique I developed called the Cold-Subfascial Breast AugmentationR. The patient related that she changes in front of other models routinely and pretty much all of them look like she did. She was however interested in a revision after seeing the typical results with Cold-Subfascial Breast Augmentation. Revision from dual-plane or sub muscular is possible because the complete fascia is usually intact and window shades up with the muscle. In revision the muscle is returned to its natural anatomic position and the fascia is used to support the implant. I revised her and delivered a softer, more centralized and supported result as depicted below:

Revision of a dual-plane breast augmentation to a Cold-Subfascial Breast Augmentation

Revision of a dual-plane breast augmentation to a Cold-Subfascial Breast Augmentation
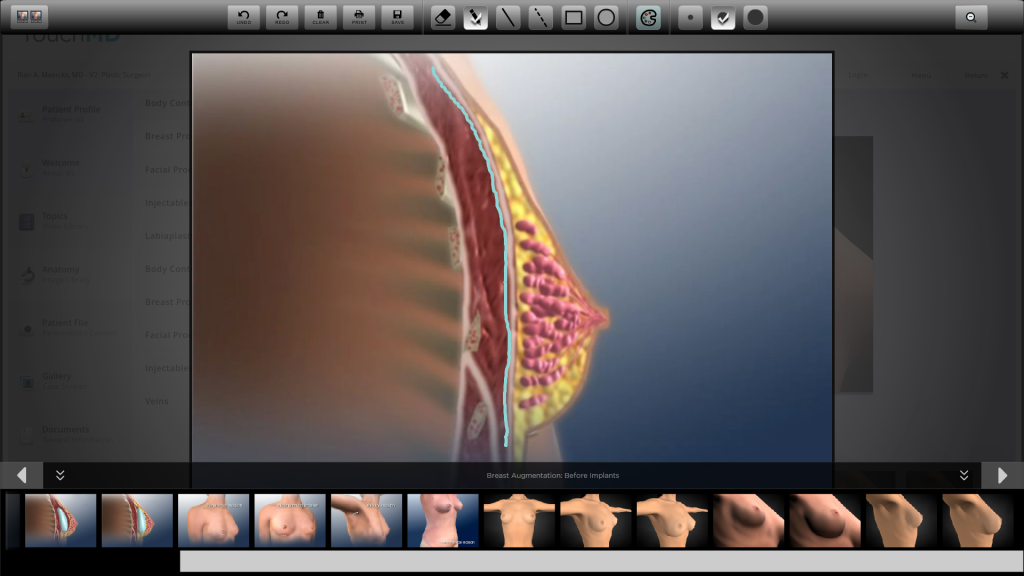
To understand the difference lets look at some more illustrations. Overlying all muscles is a layer called fascia. Fascia is strong connective tissue that condenses into tendons which allow muscles to concentrate force and pull. It is the white stripe identified in cross section below.
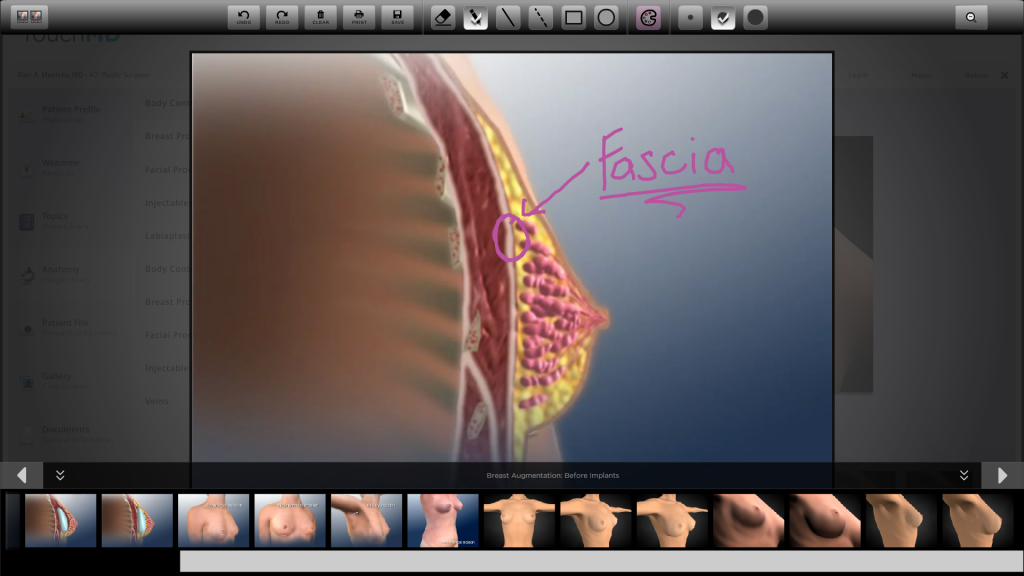
The pectoral fascia used in subfascial breast augmentation
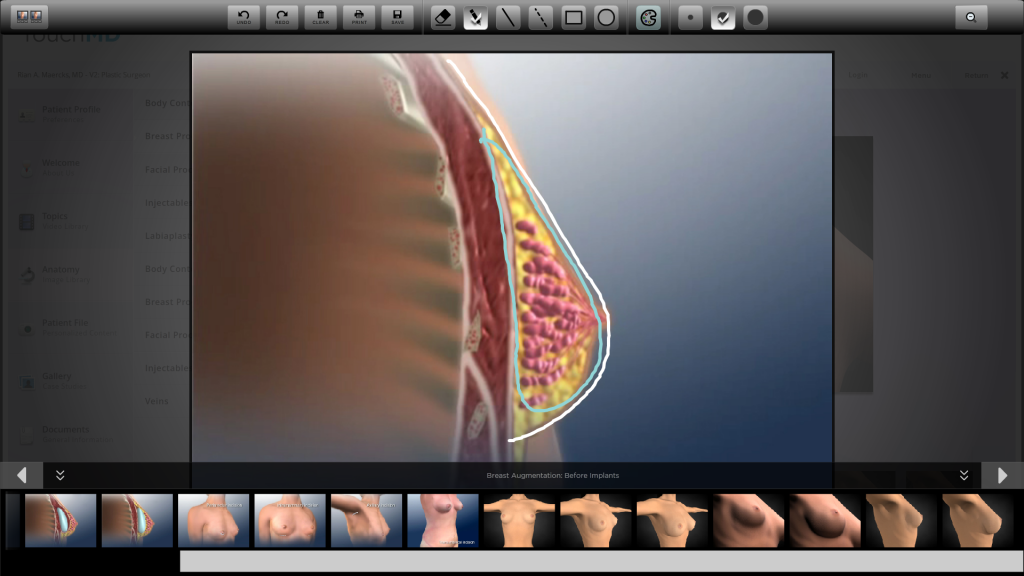
In Cold-Subfascial Breast Augmentation, I dissect the fascia away from the muscle, as depicted by the blue line below, lifting this structure intact to be used as a shaping and supporting structure for the breast augmentation. The muscle itself stays preserved in its natural anatomic position.
I dissect the fascia to create essentially a supporting and shaping support bra inside the breast. The dissection allows control over the placement and dimensions of the implant.
I place the implant depicted in blue inside this “sculpted support bra” to achieve soft sloping shapes. I select low profile anatomically shaped implants to support the cause of creating a natural shape. This allows me to achieve true superior pole fullness that appears soft and natural and also to create a “soft start” of the breast just next to midline. The width afforded by lower profile devices also allows me to create the subtle projection of the breast just lateral to chest wall to create an elegant female silhuoette.
The small amount of subcutaneous tissue depicted in yellow tends to come up with the fascia redraping and achieving a soft teardrop like effect of a natural breast.
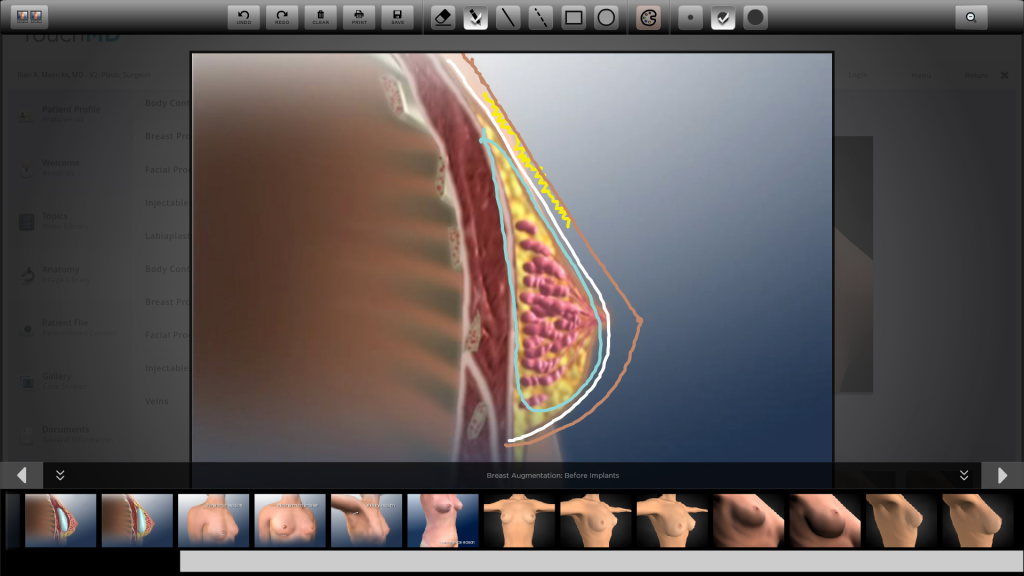
Creation of a natural appearing tear-drop shape in Cold-Subfascial Breast Augmentation
Lets compare this with what we know of subpectoral dual-plane augmentation. Below we see the flattening effect of the pectoralis major muscle on a round projecting implant. It creates the recognizable “augmented look” that I really don’t believe many women would chose if given a choice.
The flattening forces of the pectorals major muscle in dual-plane sub muscular breast augmentation leading to the fake, unnatural “augmented” look
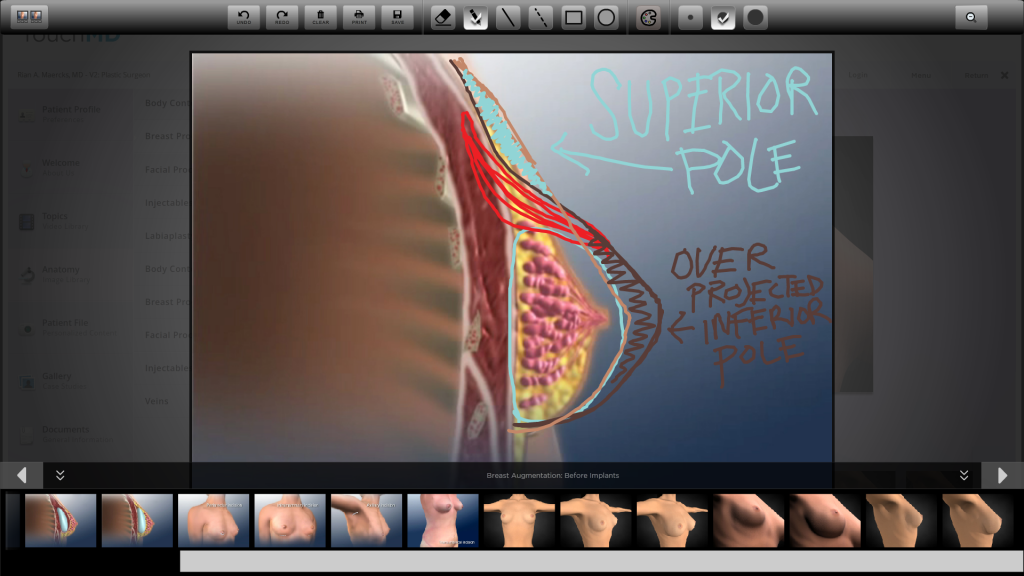
If we contrast the different approaches in profile, we will see that conventional techniques(dark brown profile) and practices lead to a small focused projection(extra brown area) that is surrounded by contrasting flatness- the augmented look. What I consider to be a more natural look, that of the Cold-Subfascial Breast Augmentation is a less projected(light brown profile) form that occupies the true aesthetic “real-estate” of the breast both centrally laterally and very importantly creating true superior pole fullness (light blue hatched area).
The secondary advantages of the subfascial plane are that the implant not only is free from the displacing forces of the pectoralis major muscle, but the axillary fold is also not altered. When the pectoralis major muscle is cut in dual-plane augmenation the axillary fold rises creating what I call axillary breast disjunction. This creates the appearance of a fatty collection near the armpit that bothers most women. Having the muscle in its native position also prevents the distracting “muscle jumping” or muscular animation seen in dual plane breast augmentations when women move their arms.

COLD-SUBFASCIAL BREAST AUGMENTATION natural appearing results. The picture to the left exhibits naturally occurring pectoral-breast disjunction causing the appearance of loose fatty tissue near the armpit. Dula-plane techniques tend to exaggerate this by raising the axillary fold when the muscle is cut and lowering the appearance of the breast. The Cold-Subfascial result to the right demonstrates that by leaving the muscle in its native position and achieving true superior pole fullness the disjunction disappears.
I hope that thus far I have demonstrated that there is a dogmatically indoctrinated acceptance of sub muscular “augmented” looking breasts among surgeons and patients alike. Now I would like to demonstrate how this conception and technique lends itself to selection of implants that can never deliver natural appearing results.
Consider the two implants below, which one is larger?


Contrasting appearance of a projection round 500mL implant that is most commonly used in breast augmentation and a low profile anatomically shaped 500mL implant used in Cold-Subfascial Breast Augmentation
You probably like most viewers out there picked the one on the left to be the larger one. The fact is they are both the same exact size. They are both 500mL implants. The one on the left is the style most commonly used, the type of implant all plastic surgeons are trained to use in residency myself included. They are round and projecting, pushing out on their own (see my blog entitled “the aesthetic evil of push”). They look big because all the volume is concentrated on a small narrow base. The implant on the right is an Allergan 410FM style implant, the line that I most commonly use which is the lowest profile anatomically shaped implant on the market. It doesn’t appear to be huge because it has a much wider and taller footprint. I select these because they allow me to fill out the true aesthetic dimensions of the breast. You are probably thinking why the heck don’t more surgeons use these in light of what was discussed above and the answer is that they can’t.
Recall the illustration above demonstrating how the dissected muscle of the dual-plane technique limits how close the implant can get to midline. This limits the width of the implant that can be used. Similarly height is limited because the muscle will use additional height to push down further cramping the implant even lower in the inferior pole. The restricted footprint of the dual-plane breast augmentation requires use of narrower shorter implants thus projection is turned to for increases in size. Unfortunately the result is a breast that is aesthetically too narrow for the chest wall and overprotection that leads to more muscular force down and out.
One of the many beautiful aspects of subfascial breast augmentation is that the ideal aesthetic breast footprint can be created in most patients creating a harmonious shape that appears made by nature.
Alright so why doesn’t everyone perform subfascial breast augmentation?
There are many reasons perhaps most importantly is that it is not taught in training. As a matter of fact in my training I was told that transaxillary breast augmentation was impossible with silicone implants, transaxillary revision was impossible and the subfascial plane does not exist. All of these procedures are core elements of my current practice. A true subfascial augmentation particularly transaxillary (through the armpit) takes a more advanced skill set.
Learn More About Cold Sub-fascial Breast Augmentation
Placing an implant under the muscle is very easy. The plane between the pestoralis major muscle and the chest wall is what we call a “loose areolar plane.” What this means is that it is a potential space, if you were to place a straw in this plane and blow it would instantly open up as it has no structures binding it. When a surgeon performs a sub muscular breast augmentation, a small hole is made in the muscle, a finger is inserted into this potential space and with a quick sweeping of the finger most of the dissection is completed.
There is no potential space between the pectoral fascia and the pectorals major muscle. It is tightly bound. Thus when a true subfascial fascia preserving technique is performed such as the Cold-Subfascial technique, there is meticulous dissection required. I perform the entire procedure under direct visualization using lighted retractors and all sharp instruments like scalpel and facelift scissors. It is a different beast. It is very unlikey for a surgeon who has had years of success with a much easier procedure to adopt a more difficult one.
Another key feature to realize is that although strong, the pectoral fascia is very thin and laminar. This means that if high power electrocautery is used in dissection much of the fascia is vaporized and if blunt dissection is used the fascia is delaminated and weakened. I think this explains why so many with heavy general surgery mastectomy backgrounds will say that the fascia doesn’t exist, they are used to vaporizing it with high powered cautery in mastectomies. This is one of many reasons why I developed the Cold-Subfascial technique. The fascia itself is well studied with many anatomic dissections and structural characterizations in the published literature.
More on this to come in future blogs. I hope that I have demonstrated why the augmented look exists and why it is so well tolerated. More natural and beautiful results are attainable safely and efficaciously but is very unlikely to ever be mainstream. Thanks for reading! If you have questions or suggestions for future blogs I am all ears. Drop a note through this website or the Facebook page. Until next week…
Rian A. Maercks M.D.
Aesthetic, Craniofacial and Reconstructive Plastic Surgery
305.328.8256
